





Scoliosis & Spinal Deformity Correction
Experts in Scoliosis Surgery

Scoliosis is a fairly common medical condition in which the spine has an abnormal curvature. Depending on the degree of the abnormal curvature, scoliosis may be either negligible or a constant obstacle to everyday activity and to vital organs.
There has been a great deal of research into the condition, however, and a range of treatments has been developed. Surgery is the solution when is the curve more than 40 degrees. There are several approaches to perform scoliosis surgery.
Traditional approaches involve making long incision over the curve to be corrected and cutting and retraction the muscles and tissues over the spine to gain access to the vertebra that need to be fused. It is a very major surgery with huge negative impact over the body.
With advancements and innovations in minimal invasive surgical techniques, we can achieve the same goals as traditional surgery, yet with much less trauma to the surrounding muscles and tissues through minimal invasive scoliosis surgery. Using a few small incisions instead of a single large one, and also using muscle sparing surgical approaches, many scoliosis curves can be reconstructed with similar results to traditional open approaches.
The real advantages of minimally invasive instrumentation are better cosmesis, less pain, shorter hospital stay, faster return of function. Our target to change the high impact negative surgery to easy less traumatic without pain, bleeding, big scars, and with fast recovery and good quality of life.

Dr. Firas M. Husban
Consultant Orthopedic Surgeon
Nationality : Jordan
Years of Experience : 25
Expertise

Dr. Shahid Khan
Consultant Orthopedic Surgeon
Years of Experience : 15
Nationality : UK
Expertise

Thoracic
The thoracic spine is the longest region of the spine, and by some measures it is also the most complex. Connecting with the cervical spine above and the lumbar spine below, the thoracic spine runs from the base of the neck down to the abdomen. It is the only spinal region attached to the rib cage.

Thoracolumbar
Neurological deficits suggesting trauma to the spinal cord in the thoracolumbar area are the most common clinical presentation of neurosurgical conditions. By far, the most common cause of thoracolumbar spinal cord dysfunction is intervertebral disc disease.
Lumbar
The lumbar spine refers to the lower back, where the spine curves inward toward the abdomen. It starts about five or six inches below the shoulder blades, and connects with the thoracic spine at the top and extends downward to the sacral spine.
Degenerated Discs Intervertebral discs are spongy pads that act as shock absorbers between each of the lumbar spine’s vertebrae. Disc degeneration can create pain in the disc space. This condition can be referred to with many different terms – on this site it is consistently termed “degenerative disc disease.”
Lumbar Disc Herniation Herniated discs are most common in the lumbar spine. A herniated disc may happen suddenly due to injury or heavy lifting or happen slowly as a part of general wear and tear on the spine. Leg pain (sciatica) is the most common symptom of a herniated disc.
Sacroiliac Joint Dysfunction The sacroiliac joint, which connects with the bottom of the lumbar spine and the top of the tailbone, can cause lower back pain and/or sciatica pain if there is any type of dysfunction in the joint that allows too much movement or restricts normal movement.

Double Curve
Although the spine does curve from front to back it should not curve sideways very much. A side-to-side curve is called scoliosis and may take the shape of an “S” (double curve) or a long “C” (single curve).
The exact cause of double curve scoliosis is unknown, but this condition is not uncommon, nor is it life-threatening. While both curves will usually be of roughly equal size, a double scoliosis patient’s Cobb angles may be anywhere from 10 degrees to 100 degrees.
As this spinal condition progresses, back pain can develop and the curvature can put pressure on your nerves. This can lead to weakness, numbness and pain in your legs, and may even cause a loss of coordination in the muscles of the legs, making it difficult to walk.In severe cases, the patient’s lungs or heart may be affected, leading to breathing problems and heart failure. Luckily, such extreme outcomes are very rare even if you do have an ‘S’-shaped spine.· One of your hips or shoulders being higher than the other· One of your shoulder blades being higher or sticking out further than the other· A rib hump (if your scoliosis has caused your chest to become twisted)· One arm appearing to be longer than the other because of a tilt in your upper body
As this spinal condition progresses, back pain can develop and the curvature can put pressure on your nerves. This can lead to weakness, numbness and pain in your legs, and may even cause a loss of coordination in the muscles of the legs, making it difficult to walk.In severe cases, the patient’s lungs or heart may be affected, leading to breathing problems and heart failure. Luckily, such extreme outcomes are very rare even if you do have an ‘S’-shaped spine.
Some curves do not respond to bracing despite everyone’s best efforts, and some curves are just too large to begin with (greater than 45-50 degrees). If your child has this type of curve, he/she may need surgery. If your child’s health care provider recommends surgery, you’ll want to think about it seriously and ask many questions. The goal of the surgery is a usually a solid fusion (stabilization) of the curved part of the spine. A fusion is achieved by operating on the spine, adding bone chips and allowing the vertebral bones and bone chips to slowly heal together to form a solid mass of bone called a fusion. The bone chips (bone graft) may come from a bone bank or your hip (iliac crest).
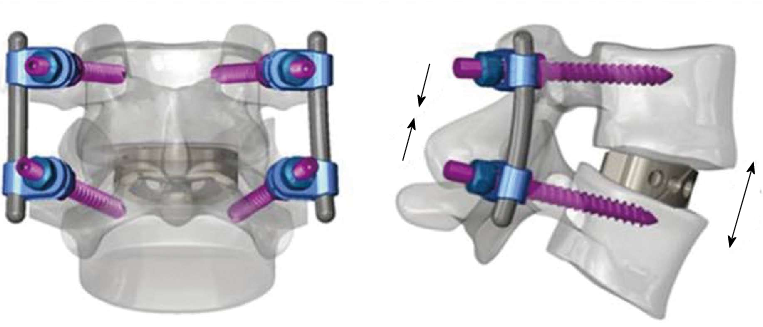
Usually, the spine is substantially straightened with metal rods and hooks, wires or screws(instrumentation). The rods hold the spine in place until your child’s fusion has a chance to heal. Once the fusion has healed (usually 3 to 12 months) the abnormal section of the spine cannot curve more. The rods, hooks or wires are usually left in your child’s back without causing any problems. Surgery varies greatly depending upon the amount of spine fused and your child may or may not experience a noticeable loss of spinal motion. Your child’s health care provider can tell you what activities he/she can do after a spinal fusion. Most sports are possible after a spinal fusion.

Posterior Fusion
Posterior fusion with instrumentation is the most common operation done for idiopathic scoliosis. In the posterior fusion the spine is operated on from behind with an incision straight down the back. Various types of rods, hooks, wires or screws are used to partially straighten the spine and hold it fast while the bone fusion occurs. For most of these operations on idiopathic scoliosis, no brace or cast is used postoperatively. In some congenital scoliosis or spondylolisthesis the posterior fusion may be done without instrumentation, and a brace is needed postoperatively.

Posterior Fusion
Posterior fusion with instrumentation is the most common operation done for idiopathic scoliosis. In the posterior fusion, the spine is operated on from behind with an incision straight down the back. Various types of rods, hooks, wires, or screws are used to partially straighten the spine and hold it fast while bone fusion occurs. For most of these operations on idiopathic scoliosis, no brace or cast is used postoperatively. In some cases of congenital scoliosis or spondylolisthesis, the posterior fusion may be done without instrumentation, and a brace is needed postoperatively.
Anterior and Posterior Fusion
Some special cases of spinal deformity require both an anterior (front) and posterior (back) operation. Usually, these can be done on the same day, but sometimes they must be done at separate operations.

Growing Rods
MAGEC™ (MAGnetic Expansion Control) or VEPTR™ (vertical expandable prosthetic titanium rib). Sometimes stabilization of a curved spine is needed at an age too young to be fused. In very young patients, rods can be attached to the spine (growing rods) or ribs (VEPTR) and periodically lengthened to keep up with spinal growth. Rod lengthening can be done with a small day surgery procedure or sometimes just using a magnetically driven rod (MagEC) without surgery. At an older age, a spinal fusion can be done.

